
Unopposed Alpha Vasoconstriction/Unopposed Alpha Agonism
What causes the hypertensive reaction?
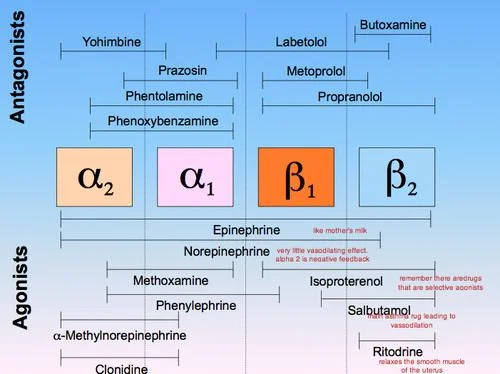
In the absence of beta-blockade, a systemic dose of epinephrine does not have much effect on mean blood pressure because it has both alpha-adrenergic effects (producing vasoconstriction) and beta-adrenergic effects (producing vasodilation). If a patient on a non-selective beta-blocker receives a systemic dose of epinephrine, the non-selective beta-blocker prevents vasodilation, leaving unopposed alpha vasoconstriction (also termed unopposed alpha agonism). The hypertensive reaction can be considerable, with a systolic pressure well over 200 mm Hg.
Do all beta-blockers increase the risk of acute hypertension?
No. Cardio-selective beta-blockers, such as acebutolol, atenolol, betaxolol, bisoprolol, esmolol, and metoprolol, would not be expected to cause hypertensive reactions following a systemic dose of epinephrine. This is because cardio selective beta-blockers have little effect on the beta-adrenergic receptors in the arterioles. Nonetheless, one should consider the possibility of an interaction of epinephrine with cardio-selective beta-blockers if plasma concentrations of the beta-blocker are elevated due to large doses or other factors.
Is the dose of the epinephrine important?
Yes. The small amounts of epinephrine (combined with local anesthetics) that may be used in routine are unlikely to be a problem.
Specific Anesthesia Considerations for the Burn Patient Undergoing Surgery, Regarding Beta-Blockade & Epinephrine Administration
Tangential excision is the meticulous removal of burned skin while preserving the underlying viable tissue. Bleeding is intentionally created by burn surgeons to not only remove the burned tissue but also to ensure an adequate vascular bed is present for the grafting and healing process. Once the surgical area is successfully excised and bleeding is established, the epinephrine soaked telfa pads are applied to achieve hemostasis. The epinephrine soaked telfa’s are created by the scrub nurse/tech. She/he soaks approximately 30 to 50 telfa’s in one liter of warmed normal saline mixed with 90 mg of epinephrine. It is not uncommon for three or four liters of the saline and epinephrine mixture to be applied to the wound bed(s) by the surgeon during the case. Think of what one mg of epinephrine does when administered. Now 270 to 360 mgs of epinephrine are being applied to a fresh, bleeding vascular bed. If an adequate and balanced anesthetic is not achieved prior to the application of the epinephrine soaked telfa’s, profound hypertension and tachycardia may result. If this occurs consider increasing narcotic administration, increasing volatile agent/TIVA delivery and/or asking the surgical team to remove the telfa’s until acceptable hemodynamics are achieved before continuing. Cardio-selective beta-blockers have their place, but should not be the first line of attack to correct this abnormal hemodynamic situation. If you do decide to commit to a vasoactive agent, consider its half-life, since the epinephrine effects are usually gone within 60 to 90 minutes after surgical application.
Horn, J. R., PharmD, FCCP, & Hansten, P. D., Pharm D. (2009, May 15). The Dangers of Beta-Blockers and Epinephrine. Retrieved November 4, 2018, from https://www.pharmacytimes.com/publications/issue/2009/2009-05/druginteractionsbetablockers-0509